Early Identification of Austism Spectrum Disorder
 INTRODUCTION TO THE ONLINE MODULE
INTRODUCTION TO THE ONLINE MODULE
Hello and welcome to the Early Identification Online Module developed by the National Professional Development Center on ASD.
As you may already know, the number of children diagnosed with autism has risen dramatically over the past few decades. In 2007, the Center for Disease Control and Prevention (CDC) estimated the prevalence of autism spectrum disorder (ASD) as 1 out of every 150 children.
This finding was informed by data collected in multiple communities throughout the U.S. in 2006 by the CDC’s Autism and Developmental Disabilities Monitoring (ADDM) Network. The study reported an average age of diagnosis at 4-1/2 years of age, with boys being four to five times more likely than girls to have an ASD. While ASD has been found in all racial, ethnic and socioeconomic groups, there are unanswered questions about potential racial and ethnic disparities (Cuccaro et al., 1996; Mandell et al., 2009). Further study may reveal the prevalence to be higher.
Autism spectrum disorder (ASD) is the umbrella term used to describe several different conditions.
These include Autistic Disorder, Asperger’s Disorder, and Pervasive Development Disorder-Not Otherwise Specified (PDD-NOS). ASD will be used throughout this website and online module.
In the last decade, we have made a great deal of progress in recognizing autism in young children, but there is still a long way to go. Although signs of autism are usually present by the second birthday and a third of parents cite first concerns about their child’s development prior to the first birthday (De Giacomo, & Fombonne, 1998), clinical diagnoses are not typically made until the fourth year of life or later (Mandell, Novak, & Zubritsky, 2005). Early identification and treatment are central to positive outcomes for children with autism as they grow and develop ( Rogers, 1996; Smith, Groen, & Wynn, 2000).
Let's improve the important task of early identification of ASD, because the earlier we can recognize the signs, the earlier we can start treatment.
Before you begin the module, take a Pre-Assessment Quiz
Module Contents
Early Identification of ASD Online Module
Importance of Early Identification of ASD
Characteristics of ASD in Young Children
![]() Videos of Early Identification of ASD Onset
Videos of Early Identification of ASD Onset
Processes for Early Identification of ASD
Communicating with Parents About Screening and Diagnostic Results
Case Study
Additional Resources for Early Identification
Summary
Module Objectives
After completing this module, you will be able to:
-
Describe barriers to early identification
-
Describe the importance of early identification and early intervention
-
Distinguish between screening and diagnosis of autism
-
List three components of the American Academy of Pediatrics’ 2007 guidelines for universal screening for autism
-
List early red flags for autism in the infancy and toddler years (before age 3)
-
Describe different patterns of onset of autism
-
Name three screening measures for autism and describe their strengths and weaknesses
-
Name three diagnostic assessment measures for autism and describe their strengths and weaknesses.
-
Describe three considerations for communicating screening and diagnostic assessment results to parents.
- Name three national organizations or agencies that have resources to support early identification of autism.
Pre-Assessment Quiz
| Questions: | 8 |
| Available: | Always |
| Pass rate: | 75 % |
| Backwards navigation: | Forbidden |
Pre-assessment Quiz
Select the Start Quiz button to take the pre-assessment for the module.
This pre-assessment quiz contains eight true/false and multiple choice questions.
After the quiz, you will begin learning about the Importance of Early Identification of ASD.
Importance of Early Identification
What are the potential benefits to early diagnosis of ASD?
 Benefits for Families
Benefits for Families
Selecting Appropriate Treatments
Societal Cost of ASD
Family Benefits of Early Identification of ASD
First, diagnosing autism as soon as possible gives families some answers they are seeking to their questions about their children’s atypical development. This allows them to begin the process of learning about autism, understanding its effects on their child, and beginning the process of perceiving the future differently. It allows families to replace worry and fantasy with solid information about the nature of their child’s challenges. For many families, receiving a diagnosis allows them to move from unfocused worry to mobilized efforts to learn about the disorder, to find help for their child, and to move into some action plan; such mobilization is often a source of relief from some of the anxiety parents experience as they move through the diagnostic process.
Better Outcomes for Young Children with ASD
The second potential benefit of early diagnosis has to do with selection of appropriate treatment strategies. Children with autism have a different learning profile pattern of relative strengths and weaknesses than children with other developmental disorder. Thus, it is not surprising that children with autism learn most rapidly when they receive unique teaching and curriculum approaches, approaches built for their distinctive learning profile. These methods for teaching young children with autism contain elements that are not seen in early intervention approaches for young children with other kinds of disabilities. Specifically, there is more focus on direct instruction, higher levels of structure, higher numbers of intervention hours per week, and lower child to teacher ratios than are typically seen in early intervention services in most communities for children with other developmental problems. A number of studies have documented better outcomes for young children with autism who receive intensive and specialized treatment as early as possible (Hoyson, Jamison, & Strain, 1984; McEachin, Smith, & Lovaas, 1993; Rogers, & Lewis, 1989; Sheinkopf, & Siegel, 1998; Dawson et al., 2010). Some of these studies have demonstrated considerable IQ and speech gains and much better functioning in elementary school for children receiving intensive and specialized intervention by age 3. Thus, earlier diagnosis allows the most appropriate treatment to be selected and delivered.
Reduce Impact of ASD on Societal Costs
Finally, the lifetime societal cost of autism, including care and lost productivity, has been estimated at $3.2 million per child (Ganz, 2007), with health care expenditures increasing sharply (142%) over the last five years (Leslie, & Martin, 2007). Therefore, it is critical to the individual, the family, and even to society that we improve our efforts at early detection and access to early intervention in order to attempt to lessen the impact of the disability associated with autism.
Characteristics of ASD in Young Children
DSM-IV Criteria and Early Diagnosis
Children with autism and ASD over the age of 3 generally display characteristics of autism that map well onto the diagnostic criteria outlined in the Diagnostic and Statistical Manual of Mental Disorder (DSM-IV) (2000). It is not clear that DSM-IV criteria are equally applicable to children under age 3 and particularly younger than 2, however. Stone and colleagues (1999) have examined this question empirically in a group of two-year-olds diagnosed clinically with autism.
DC:03R and Early Characteristics of ASD
To address concerns about the difficulties with the DSM-IV for the early childhood years, the Diagnostic Classification of Mental Health and Developmental disorder of Infancy and Early Childhood: Revised Edition (DC:0-3R) (2005) was developed and published by the Zero to Three organization. It is an evolving classification system that is based on expert consensus rather than empirical findings and is designed to complement, not replace the DSM-IV in identifying early mental health and developmental difficulties in children under the age of five. The classification system adds additional diagnostic categories not found in DSM-IV, for the purpose of clinical guidance and more detailed description of early childhood difficulties. Since it has not been empirically validated, it should not be substituted for the DSM-IV as a diagnostic standard for ASD.
A great deal of research has been done to explore the earliest signs of autism and when they can be detected. Several research strategies have been used to study these questions, including:
- retrospective parent interviews,
- examination of home video collected prior to diagnosis, and
- most recently, prospective studies that follow infants at risk for autism through the window of time when autism emerges.
Strong consensus has been obtained across all research methods. Behaviors that consistently discriminate infants or toddlers with autism from those with non-autism developmental delays or typical development are orienting to name, eye contact, social referencing, interest in other children, joint attention, affect sharing, and imitation (see Rogers, 2009 for a review).
A 2010 study (Ozonoff et al.) that compared siblings of children diagnosed with ASD and typically developing infants found that the earliest characteristics of autism are not readily observed at six months, but emerge gradually between nine and twelve months of age. Observed characteristics, such as a lack of shared eye contact, smiling and communicative babbling, contribute to the consensus reached by previous research.
Onset Patterns: Two Videos
Onset Patterns
Recently, our understanding of how the first signs of autism emerge has changed. The traditional notion was that there were two broad onset patterns.
The most common course involves early signs of developmental differences, before 12-18 months of age. In approximately a third of cases, however, symptom onset does not occur until sometime in the second year of life, between 14 and 24 months of age (Fombonne, & Chakrabarti, 2001; Lord, Shulman, & DiLavore, 2004), after a developmental regression, or loss of previously acquired skills. The most frequently reported skill lost is language, although virtually all children who lose language lose social behaviors as well, such as eye contact, social interest, and engagement with others (Ozonoff, Williams, & Landa, 2005). However, more recently, we have come to realize that these two onset patterns do not capture all of the different ways autism emerges.
There seem to be different patterns of late onset of symptoms - regression and plateau - though it is often difficult to separate children who show a regression (skill loss) from children who show a developmental “plateau,” marked by a failure to progress and transform simpler behaviors into more advanced social and communication skills (Chawarska et al., 2007; Siperstein, & Volkmar, 2004). Moreover, many children with a reported regression already have a number of developmental delays prior to the regression itself (Goldberg, Thorsen, Osann, & Spence, 2007; Ozonoff et al., 2005; Siperstein, & Volkmar, 2004; Werner, Dawson, Munson, & Osterling, 2005), and some children with clear signs of autism in the first year of life also experience skill loss in the second year (Werner, & Dawson, 2005).
Some have suggested four different onset patterns: early (before 12 months) onset of symptoms without skill loss, late onset of symptoms seen in skill loss (regression) without early symptoms, early onset combined with later skill loss, and late onset without skill loss (developmental plateau) (Ozonoff et al., 2010).
Another way to think about how autism begins is that children may reach the threshold for diagnosis at different points in the first three years of life, involving different amounts and/or combinations of early signs, slowing development, lack of progression, and frank losses (Landa et al., 2007; Rogers, 2009; Ozonoff et al., 2010).
View two videos that illustrate the two traditionally defined patterns of onset:
Video 1: Onset in the First Year of Life
Video 2: Onser After Regression
Remember that not all children will fall into these categories or that failure to display these kinds of trajectories does not rule out an autism diagnosis.
Video 1: Onset in the First Year of Life
Duration: 3 minutes
Video 2: Onset After Regression
Duration: 4 minutes, 18 seconds
Surveillance, Screening, and Diagnosis for Early Identification of ASD
Surveillance, Screening, and Diagnosis for Early Identification of ASD
There is considerable need for further research, innovation, and improvement in early identification, given the gap between the age when ASD characteristics are first noticed and when a diagnosis is made, as Shattuck et al. (2009) suggested. There are several levels of recommended practices that lead to the early identification of ASD.
Surveillance is the ongoing process of identifying children at risk. Surveillance methods are often simply questions that primary care providers ask all parents at well-child visits about developmental milestones.
Screening is a brief assessment that uses standardized instruments to identify children at significant risk of having a disorder. The results of screening indicate the presence of risk characteristics for delay or disability, but do not provide a diagnosis.
Diagnostic assessment involves a detailed assessment process using standardized tools, observations, and clinical history to define the child’s difficulties and determine the presence of a clinical diagnosis. A diagnostic assessment is the final step in early identification of a specific disorder.

The American Academy of Pediatrics endorsed new practice parameters for ASD screening and evaluation to occur with primary care pediatric practices as summarized in Identification and Evaluation of Children with Autism Spectrum Disorder (Johnson et al., 2007).
Download PDF: http://pediatrics.aappublications.org/content/120/5/1183.full.pdf
There are several new early identification guidelines laid out in this document, which represents a significant new milestone for the autism field.
Among the most important recommendations are the following:
Primary care providers should become aware of early signs of ASD;
Primary care providers should routinely ask all parents about developmental milestones and behavior at each visit; If any concerns are identified by parents or professionals, an autism-specific screener should be administered and/or the child should be immediately referred for a diagnostic evaluation, depending upon the level of concern;
Primary care providers should screen all children, using an autism-specific screener, at 18 and 24 months of age.
These autism specific refinements follow previously established parameters for the universal screening of all children for potential developmental delays at 9, 18 and 24 (or 30) months during well-child visits. This surveillance and screening algorithm can be found at the National Center for Medical Home Implementation website.
Continue for more information on Surveillance, Screening, and Diagnostic Assessments
Communicating Screening and Diagnostic Results with Parents
Communication of findings to parents is an essential part of early identification and diagnosis of ASD.
Parents are often the first to recognize that something is different in their child’s development. By the time surveillance and screening is conducted, some parents may have already had concerns about their child’s development. It is important to consider a parent’s perceptions when discussing with them your developmental concerns and questions about red flags for ASD. The direction of a conversation might progress differently with a parent who has already been wondering if their child is showing characteristics of ASD compared to a parent who has not considered the possibility.
If you are a professional, for a parent with questions about their child’s development, start a conversation with recognition of the concerns followed by queries for more detailed descriptions. If a physician, child care provider, or other family member first notices the concerns, the conversation would start differently.
The conversation might start with a statement of concern, such as, “I’ve noticed that your child isn’t showing an interest in what you are experiencing together. Have you noticed this?”
Allow for exchanges with families within context of conversations
These scenarios create a context for those conversations that provide exchanges with families, rather than reporting to families, within which a diagnosis of ASD is delivered.
Choose language carefully
It is important to choose language carefully and give a clear message about the findings. If further evaluation is recommended due to concerning screening results, say so. If a diagnostic assessment indicates the diagnosis of autism, say so. Concurrently, if a screening or diagnostic assessment indicates no concerns, it is equally important to assure parents that their child’s development is on track with typical development or to highlight concerns for future follow up.
Be prepared for parents' emotional responses
Parents will have a range of emotional responses to new developmental or diagnostic information about their child.
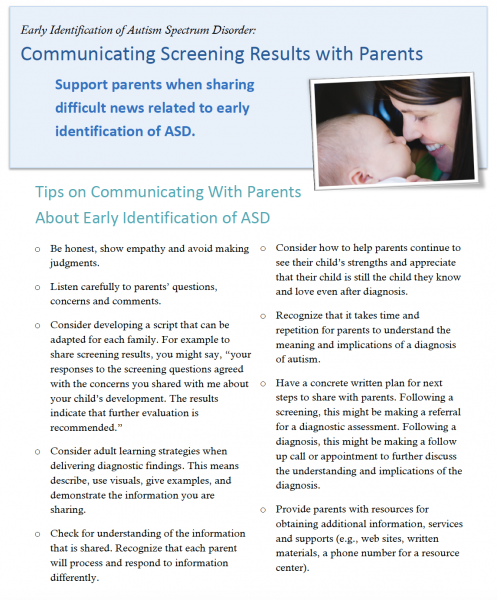
Support parents when sharing difficult news related to early identification of ASD.
View Tips on Communicating Screening Results with Parents
For more guidance, view this video webcast form the Wisconsin Medical Home Webcast Series.
Sharing Screening Results with Families
Website URL: http://www.waisman.wisc.edu/connections/webcast.php
{kind=link}
Case Study
Case Study: Early Identification of ASD Surveillance and Screening
This case study demonstrates how the processes of surveillance and screening begin during a visit to a primary care physician and result in referral for additional evaluation, diagnosis, and intervention. You may test your learning by answering the questions provided.
 ALEX
ALEX
Alex is a 16-month-old boy who is at the pediatrician’s office for an ear infection. In passing, his parents mention that they are also concerned that he isn’t yet speaking.
What should the pediatrician do next?
The pediatrician asks Alex’s parents a few questions, such as whether he responds to his name and enjoys social games. They respond that he likes to play peek-a-boo with them, but that it can be hard to get his attention by calling his name.
What other questions might the pediatrician ask?
The doctor also asks about Alex’s babbling and whether he uses gestures like pointing to get his needs met.
What screening tool would you use to assess Alex’s risk of autism?
The pediatrician asks Alex’s parents to fill out an autism-specific screener, the M-CHAT. His score is right at the cutoff for “high risk.”
What should the pediatrician do?
The pediatrician refers Alex to the Part C early intervention program so that he may start services as early as possible, regardless of a diagnosis. Concurrently, she made a referral to a community program/clinic for toddlers with potential developmental difficulties, including autism, The purpose of the later referral was to request a comprehensive developmental evaluation to begin the diagnostic process for a potential autism spectrum disorder. She also refers Alex to an audiologist to have his hearing tested.
What should the pediatrician be cautious about?
-
Diagnoses should not be made on the basis of screening tests alone.
-
As you will learn in this module, signs of autism often emerge slowly during the first 18 months of life. The clinical presentation is not always as clear as it is in older children.
-
It is important for a professional with expertise in the earliest signs of autism to perform the comprehensive evaluation, using validated instruments appropriate for Alex’s developmental level.
-
Many more children who fail screening tests will have communication delays (e.g., speech delays) than autism.
-
The stability of diagnosis prior to age 3 is good, but not as good as after age 3. Therefore, it is important that any child diagnosed before 3 years be re-assessed after this age to examine the accuracy of diagnosis. Also, parents should be told that there is some diagnostic uncertainty at this age.
What happened to Alex following this?
The early intervention program found Alex eligible for early intervention services, resources, and supports due to delays in his language development and differences in his social relatedness with others.
As Alex’s second birthday approached, the early signs identified on the M-CHAT became more pronounced, plus other characteristics of ASD were emerging. The comprehensive evaluation resulted in an initial diagnosis of autism.
Recommendation for re-evaluation was suggested when Alex turned three. The family was given information about intensive services that Alex may benefit from in addition to those he received through the Part C early intervention program. The audiologist did not find a permanent hearing loss, but found that he had some fluid in his ears that may have been causing some interference with his hearing.
Summary
Summary of Early Identification of ASD Online Module
- Understanding and recognizing the earliest characteristics of ASD is important to early identification and referral for appropriate services, resources, and supports.
- There are a series of actions – surveillance, screening, and diagnostic assessments that may lead to the diagnosis of autism at the earliest possible age.
- The American Academy of Pediatrics recommends developmental screening for all children (surveillance) through use of a valid and sensitive screening tool at 9, 18 and 24 (or 30) months, with additional screening for ASD at 18 and 24 months.
- Diagnostic assessments include a combination of sources including parent interviews, direct observation of ASD characteristics, use of validated tools, and developmental assessment information.
- A number of autism specific instruments, such as the ADOS, ADI-R, and CARS, have sufficient sensitivity and specificity to support an ASD diagnosis, though they may lack specificity when used with children younger than 24 months.
- For children diagnosed with ASD before the age of two, re-evaluation at or after age three is recommended to assess the accuracy of the diagnosis.
- Communication of findings to parents and referral for treatment are essential parts of early identification and diagnosis of ASD.
- There are national campaigns and initiatives dedicated to early identification of ASD.
Now take the Post-Assessment Quiz
Post-assessment Quiz
| Questions: | 8 |
| Available: | Always |
| Pass rate: | 75 % |
| Backwards navigation: | Forbidden |
Post-assessment Quiz
Select the Start Quiz button to take the post-assessment for the module.
This quiz contains eight true/false and multiple choice questions.
After this quiz, you will be provided Additional Resources on Early Identification.
Remember to visit the Module Materials section for downloadable documents referenced in the online module.
Additional Resources on Early Identification
To address priorities for earlier identification of ASD, a number of national organizations and agencies have launched campaigns and established policies to promote the early identification of ASD and other developmental disabilities.
IDEA: The Individuals with Disabilities Education Improvement Act of 2004
Website: http://idea.ed.gov/
The IDEA requires each state to provide a comprehensive child find and referral system to identify children with disabilities such as autism as early as possible and to connect these children with school and community services. Child find activities are required by Part C early intervention and school systems to identify, locate, and evaluate all children in need of early intervention, special education, and related services. There is a growing awareness and emphasis on early identification and early intervention because of these federally mandated activities. In 1990, autism was added to IDEA as a category of disability to more appropriately serve children with ASD ages 3 to 22 in schools.
AAP: Academy of Pediatrics
Website: https://www.aap.org/en-us/Pages/Default.aspx
The American Academy of Pediatrics endorsed new practice parameters for ASD screening and evaluation to occur with primary care pediatric practices, as summarized in Identification and Evaluation of Children with Autism Spectrum Disorder (Johnson et al., 2007).
CDC: Center for Disease Control and Prevention
Learn the Signs. Act Early
Websites: http://www.cdc.gov/ and www.cdc.gov/ncbddd/actearly/
Concurrent with studying the growing prevalence of ASD, the Center for Disease Control and Prevention (CDC) has launched a comprehensive public awareness campaign, Learn the Signs. Act Early. The purpose of this initiative is to increase the awareness of typical child development milestones and promote “action” if delays are suspected. The importance of acting early to make a difference has resulted in outreach to key stakeholders including parents, health care professionals, early childhood educators, and policy makers. There are many free or low cost materials that are available at the Center for Disease Control and Prevention website.
The CDC-sponsored Regional Act Early Summits were an example of how many national initiatives collaborated to support sustainable, state team work with the potential to influence policy, resources, and practices to increase early identification and intervention for children with ASD and their families. For more information, visit the Association of University Centers on Disabilities (AUCD) website at: http://www.aucd.org/template/index.cfm.
ASA: Autism Society of America
Website: http://www.autism-society.org/
A leading advocacy voice in the US for autism, ASA promotes the importance of early identification because autism is a treatable condition that is known to result in improved outcomes with appropriate and early interventions.
Autism Speaks
Website: http://www.autism-society.org/
Autism Speaks is dedicated to funding global biomedical research into the causes, prevention, treatments, and cure for autism; to raising public awareness about autism and its effects on individuals, families, and society; and to bringing hope to all who deal with the hardships of this disorder. Autism Speaks developed the ASD Video Glossary, used for video clips in this module.
U.S. Department of Health and Human Services
MCHB: Maternal and Child Health Bureau
Website: http://mchb.hrsa.gov
The Maternal and Child Health Bureau (MCHB) of the U.S. Department of Health and Human Services has committed significant resources to early identification and intervention for ASD. This includes grants to University Centers for Excellence in Developmental Disabilities to enhance leadership training to future professionals committed to working with individuals with ASD and their families. MCHB also funds State Implementation Grants for Improving Services for Children and Youth with Autism Spectrum Disorder. The Autism Medical Home Service Guidelines resulted from previous MCHB funding to the National Autism Medical Home Initiative charged to demonstrate how principles of the medical home are applied to achieve early identification and intervention for children with ASD. View guidelines on the Waisman Center National Medical Home Autism Initiative website.
FAQs
Frequently Asked Questions about Early Identification and Diagnosis of ASD
1. What should or shouldn’t I do if I suspect someone has characteristics of ASD? >>
2. How do I find out about what diagnostic resources are available in my community? >>
3. Who can make a diagnosis of ASD? >>
7. What do I do if a parent questions the diagnosis of ASD for their child? >>
1. What should or shouldn't I do if I suspect someone has characteristics of ASD?
If you suspect a child has characteristics of ASD, you have an important role in informing the child’s parents of your concerns. This is best done within the context of an ongoing working relationship with the family. The most important outcome of your initial conversation should be set up as a scheduled meeting, not an informal conversation that occurs during other interactions. The purpose of your initial discussion is to explain what behaviors you have observed, why these concern you, how parents can follow up to have the characteristics evaluated, what the evaluation process may consist of, and to recommend the first step, referral to their health care professional for screening and further assessment. It may not be important, or even advisable, to raise your concern about ASD as a specific diagnosis. Whether you mention it or not depends on what you have learned about the parents questions or concerns prior to your scheduled meeting. Diagnosis is the outcome of the evaluation process. It is more useful to the family for you to list the behaviors that concern you: language, social, behavioral, developmental. To start the conversation, you could begin by describing some of the child’s strengths and positive qualities, and then following by saying something like “I have also noticed that your child……Have you seen this, too? Is this typical of behavior you see at home?” Families may or may not endorse your observations. Be careful not to enter into a debate about your perceptions of the child’s behavior, and do not press a parent to agree with your perceptions. Your job is to provide information to families about their child. It is never appropriate to make a diagnosis during an initial conversation.
The family may ask you to help identify resources for an evaluation and it is appropriate to refer the family both to their primary health care professional and to the early intervention program or school district in their community, if this hasn’t already occurred. It is important to continue to support the family and answer their questions, remembering that it is always appropriate to say “I don’t know” as an honest answer to their questions. You will likely not have answers for all of their inquiries. The outcome of your conversation will depend upon how the information fits with concerns the parent(s) may or may not already have. Raising your concerns is extremely important, whether or not the family is ready to follow up with them. If the family wants to pursue the concerns, be sure to end the conversation with a plan for follow up so the family has a plan of action to follow.
2. How do I find out about what diagnostic resources are available in my community?
One of the best ways to find out about diagnostic resources is to check with a child’s primary care physician or other medical specialists. Many major medical centers and clinics have ASD diagnostic services. In addition, there are information and resource centers or hotlines in many states that keep track of diagnostic resources within a state or community. These resources may be sponsored by Public Health or Title V (Children and Youth with Special Health Care Needs) Programs [PDF].Parent organizations (e.g., Autism Society of America, Family Voices) maintain information about diagnostic centers. In most states, the University Centers for Excellence in Developmental Disabilities (UCEDD) have ASD diagnostic services or information about the services in their state or region. Contact information for the UCEDD in each state is available at the Association of University Centers on Disabilities (AUCD) website.
School districts have responsibility for child find, ages birth to 22. For a child in the birth to 3 age range, special education personnel will be able to help families locate the early intervention services in their community, even if they aren’t provided through the school district. For children 36 months and older, a referral to the local school district would result in the offer of developmental evaluations as well as access to a group of professional who can help families locate additional resources. There are multipe ways to learn about the resources in your community; there are no wrong entry points. It is a good idea to maintain information that is current and readily accessible for two or three key resources in your community so that you can easily make these available to parents. Sometimes parents are very nervous about making the initial calls. You may consider offering to help them do so by helping them call from your office so you can be a support to them before and after the call. However, if the family wants you to make the initial calls, be sure you have the written consent of the family to share information to the source being called before you place the call yourself; otherwise you would be breaching the family’s right to confidentiality and thus violating ethical standards.
3. Who can make a diagnosis of ASD?
Professionals from medicine and clinical psychology are credentialed to diagnose ASD. At many diagnostic centers, an interdisciplinary team of professionals is headed by a physician (e.g. developmental behavioral pediatrician), psychiatrist or clinical psychologist. Other team members may include speech-language pathologists, occupational therapists, physical therapists, nurses, nutritionists, and/or social workers. Medical specialists may also be involved to address related medical concerns (e.g., neurology, genetics, and gastroenterology). Community pediatricians, psychiatrists, and neurologists frequently make the diagnosis as well. They often use an autism specific tool as well as the reports from other disciplines to support the diagnosis.
Multi-disciplinary school teams may find a child eligible for special education services with an educational, rather than medical, classification of autism. This classification is determined by a team with many of the same disciplines that are listed above, plus educators and administrators. (See Question 8 for additional information.) It is important to understand the criteria and processes developed by each state for an educational classification of autism. This is all that is needed for children to receive educational services. A medical diagnoses of ASD is NOT necessary for a child to receive services.
All diagnosis of ASD should be based on the use of the tools and strategies recommended in the early identification module.
4. Why is it important to use autism specific instruments in the context of compreshensive developmental and health assessments?
Children with a variety of developmental disorders may have some behaviors that are also seen in ASD. In order to avoid diagnostic errors, a number of diagnostic measures have been developed that have been tested and proven to differentiate ASD form other developmental difficulties. These tools help to establish standards and consistency in protocols across professionals and settings. Use of these instruments offers assurances to families that their child’s diagnosis is based on the best available tools. In addition, it is ethical professional behavior to responsibly use diagnostic labels that help a child and family access resources and services. An annotated list of these instruments is included in this module. However, diagnosis is the result of clinical judgment, not a test score. Test scores are part of the information available to the diagnostician, but diagnosis is also dependent on the child’s history, parent descriptions of child behavior across multiple environments, and direct observation of symptoms.
5. What can be done if there are long waiting periods for obtaining a diagnostic assessment appointment? Is a child eligible for services while waiting for a diagnosis?
Waiting for a diagnostic evaluation does not mean that a child and family have to go without services and resources. A diagnosis of ASD is not required to be determined eligible to receive services. A young child with characteristics of ASD may be eligible for early intervention or special education services due to delays and differences in their development. In addition, a family may obtain other services such as speech and language therapy, occupational therapy or behavioral consultation from a psychologist in a clinical setting with a referral from the child’s primary care physician. Even if there are long waiting periods for medical diagnoses, it is best to make the appointment and wait. While waiting, there are opportunities to gather information from the providers (e.g., early intervention, child care providers, special educators, therapists) already involved with the child and family that may be helpful to the diagnostic evaluation. This would include discipline specific evaluation findings as well as narrative descriptions of a child’s learning, behavior and special interests. For example, an early interventionist, therapist or child care provider could write down examples of demonstrated capabilities as well as examples of behaviors that have been troublesome.
6. How can I and/or our team be helpful to a family who has recently received a diagnosis of autism?
Be patient, compassionate and available for communication. Listen to the family’s concerns and worries. Do not be concerned if the family is rejecting the diagnosis – there is no need for you to convince them and to try to do so will limit your ability to provide help and support. As long as the family is accessing services for the child, some acceptance of the child’s needs has occurred and the family is taking appropriate steps. Each family’s timing and needs for support and information around a new diagnosis are different. It is important to discover what those are for each family without making assumptions. We often hear from parents that having someone to listen, answer questions and provide information and resources is invaluable. This approach helps to build a trusting relationship in the early days after a diagnosis of ASD. Parents also appreciate opportunities to meet other parents of children with an ASD or other diagnosis. Consider the resources in your community for connections. This may include informal connections that you may be able to set up or a referral to a program or website that specializes in parent-to-parent matches. Organizations such as the Autism Society of America, Family Voices, and Parent-to-Parent Programs have chapters in many states and communities. They are excellent resources for such support.
7. What do I do if a parent questions the diagnosis of ASD for their child?
Listen and try to understand why the diagnosis is being questioned. Try to discover if the parent needs more information or has had a difficult experience with the diagnosis process, or some related situation. Also consider if another family member (e.g., grandparent, parent) or friend may have raised questions that has led to the questioning. Often when parents are struggling with a new diagnosis, they are well aware of the concerns, but begin to second guess or excuse their concerns as part of the process of coming to terms with their child’s condition. In some instances, you may discover that the parents have good reasons for questioning the diagnosis. In this case, it may be helpful to suggest a second professional opinion. In all situations, the goal is to support the parents as they process the new information they have received about their child: listening, exploring and identifying alternative strategies helps the parent address what is causing them to question the diagnosis. At times, this may include referral to a mental health professional for counseling, especially if you perceive the situation is more complex than what you are prepared to address. In the end, it is the parent’s choice to accept or to refuse further services for their child.
8. Is a diagnosis of ASD necessary for a child to receive early intervention or special educational services?
No. A child is eligible for early intervention services, resources and supports based on documentation of a developmental delay or a diagnosed condition. A diagnosis is not required to meet eligibility criteria. To receive special education services through a public school, a child is found eligible through a team-based evaluation process that results in a special education classification. This may include the classification of autism, but the team may find a child to be eligible for special education services through another classification such as a learning disability, behavior/emotional disorder, cognitive/intellectual disability, or speech/language impairment. Once eligible, the child’s educational needs, not the classification, guide decisions about a child’s educational services and resources.
9. Does a clinical/medical diagnosis of autism and an educational classification of autism help a child access the same services, resources, and supports?
No. A clinical/medical diagnosis of autism may help a child access health care and other related services and supports. For example, in some states, a clinical/medical diagnosis of autism is required to receive intensive in-home intervention services through a publicly funded program (e.g., Medicaid) or private health insurance. The ASD clinical/medical diagnosis may also help to access other services such as respite care and other family support benefits. A medical/clinical diagnosis does not mean a child is eligible for special education services. Special education services can only be accessed when a disability is determined and the need for special education is established. The sole purpose of an educational classification is to identify eligibility for special education and related services to address the educational needs of a child.
Module Materials
Documents for Screening and Diagnosis Instruments
Table 1: Recommended Screening Instruments
Table 2: Recommended Instruments for Diagnostic Evaluation
Table 3: Measures of Autism Symptoms not used for diagnosis
REFER TO THE FOLLOWING TABLE NOTATIONS WHEN VIEWING THE TABLES FOR SCREENING AND DIAGNOSIS INSTRUMENTS
* Age Range: Inclusive (e.g., 2 – 6 years = from 2 years 0 months through 6 years 11 months)
† Training Needs:
- Minimal: little to no training required, but presumes familiarity with instrument
- Moderate: presumes prior basic interviewing/cognitive assessment training
- Intensive: additional specialized training, such as workshop attendance, suggested
Module Activities
Activity 1: Surveillance for Early Identification of ASD
The purpose of this activity is to increase your experience in observing and describing red flags for ASD in very young children. This activity is based on viewing the Autism Speaks, ASD Video Glossary at this site:
Activity 2: Screening for Early Identification of ASD
The purpose of this activity is to review and practice administering a screening tool for ASD.
Activity 3: Diagnostic Assessment
The purpose of this activity is for you to reflect upon your experiences with diagnostic assessments for ASD.
References
Module: Early Identification of Autism Spectrum Disorders
REFERENCES
American Academy of Pediatrics, Council on Children With Disabilities, Section on Developmental and Behavioral Pediatrics, Bright Futures Steering Committee, Medical Home Initiatives for Children With Special Needs Project Advisory Committee. Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening [published correction appears in Pediatrics. 2006;119:1808–1809]. Pediatrics. 2006;118:405–420
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, 4th Edition, text revision (DSM-IV-TR). Washington, D.C.: American Psychiatric Association.
Bryson, S.E., Zwaigenbaum, L., McDermott, C., Rombough, V., & Brian, J. (2008). The Autism Observation Scale for Infants: Scale development and reliability data. Journal of Autism and Developmental Disorders, 38, 731-738.
Center for Disease Control & Prevention. (2007). Prevalence of the autistic spectrum disorders (ASDs) in multiple areas of the United States, 2000 and 2002. Morbidity and Mortality Weekly Report, 56, SS 1–2.
Charman, T., Taylor, E., Drew, A., Cockerill, H., Brown, J.A., & Baird, G. (2005). Outcome at 7 years of children diagnosed with autism at age 2: Predictive validity of assessments conducted at 2 and 3 years of age and pattern of symptom change over time. Journal of Child Psychology and Psychiatry, 46(5), 500-513.
Chawarska, K., Klin, A., Paul, R., & Volkmar, F. (2007). Autism spectrum disorder in the second year: Stability and change in syndrome expression. Journal of Child Psychology and Psychiatry, 48(2),128-138.
Cohen, I.L., & Sudhalter, V. (2005). Pervasive Developmental Disorders Behavior Inventory (PDDBI) manual. Lutz, FL: PAR.
Constantino, J.N., & Gruber, C.P. (2005). Social Responsiveness Scale (SRS) manual. Los Angeles: Western Psychological Services.
Cuccaro, M.L., Wright, H.H., Rownd, C.F., & Abramson, R.K. (1996). Brief report: Professional perceptions of children with developmental difficulties: The influence of race and socioeconomic status. Journal of Autism and Developmental Disorders, 26(4), 461-469.
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greenson, J., et al. (2010). Randomized controlled trial of the Early Start Denver Model: A developmental behavioral intervention for toddlers with autism: Effects on IQ, adaptive behavior, and autism diagnosis. Pediatrics, doi/10.1542/peds.2009-0958.
DeGiacomo, A., & Fombonne, E. (1998). Parental recognition of developmental abnormalities in autism. European Child & Adolescent Psychiatry, 7(3), 131-136.
Dietz, C., Swinkels, S., van Daalen, E., van Engeland, H., & Buitelaar, J.K. (2006). Screening for autistic spectrum disorder in children aged 14-15 months: Population screening with the Early Screening of Autistic Traits questionnaire (ESAT). Journal of Autism and Developmental Disorders, 36, 713-722.
Fombonne, E., & Chakrabarti, S. (2001). No evidence for a new variant of measles-mumps-rubella-induced autism. Pediatrics, 108(4), e58.
Frankenburg, W.K., Dodds, J., Archer, P., Shapiro, H., Bresnick, B. (1992). The Denver II: A major revision and restandardization of the Denver Developmental Screening Test. Pediatrics, 89, 91-97.
Ganz, M.L. (2007). The lifetime distribution of the incremental societal costs of autism. Archives of Pediatric and Adolescent Medicine, 161(4), 343-349.
Glascoe, F. P. (1998) Parents’ Evaluations of Developmental Status. Ellsworth and Vandermeer Press, Nashville: Tennessee.
Goldberg, W.A., Thorsen, K.L., Osann, K., & Spence, M.A. (2008). Use of home videotapes to confirm parental reports of regression in autism. Journal of Autism and Developmental Disorders, 38(6),1136-1146.
Hoyson, M., Jamieson, B., & Strain, P.S. (1984). Individualized group instruction of normally developing and autistic-like children: The LENP Curriculum and Model. Journal of the Division of Early Childhood, 8, 157-172.
Individuals with Disabilities Education Improvement Act of 2004. 20 U.S.C. § 614 et seq. (2004). (reauthorization of the Individuals with Disabilities Education Act of 1990).
Johnson, C.P., Myers, S.M., & Council on Children with Disabilities. (2007). Identification and evaluation of children with autism spectrum disorders. Pediatrics, 120(5), 1183-1215.
Kleinman, J.M., Ventola, P.E., Pandey, J., Verbalis, A.D., Barton, M., Hodgson, S., et al. (2008). Diagnostic stability in very young children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 38(4), 606-615.
Landa, R.J., Holman, K.C., & Garrett-Mayer, E. (2007). Social and communication in development in toddlers with early and later diagnosis of autism spectrum disorders. Archives of General Psychiatry, 64(7), 853-864.
Leslie, D.L., & Martin, A. (2007). Health care expenditures associated with autism spectrum disorders. Archives of Pediatric and Adolescent Medicine, 161(4), 350-355.
Lord, C., Rutter, M., DiLavore, P.C., & Risi, S. (2002) Autism Diagnostic Observation Schedule. Los Angeles, CA: Western Psychological Services.
Lord, C., Shulman, C., & DiLavore, P. (2004). Regression and word loss in autistic spectrum disorders. Journal of Child Psychology and Psychiatry, 45(5), 936-955.
Mandell, D.S., Novak, M.M., & Zubritsky, C.D. (2005). Factors associated with age of diagnosis among children with autism spectrum disorders. Pediatrics, 116(6), 1480-1486.
Mandell, D.S., Wiggins, D., Carpenter, L.A., Daniels, J, DiGuidseppi, C., Durkin, M.S., Giarelli, El., Morrimer, M.J., Nicholas, J.S., Pinto-Martin, J.A., Shattuck, P.T., Thomas, K.C., Yeargin-Allsopp, M., & Kirby, R.S. (2009). Racial/ethnic disparities in the identification of children with autism spectrum disorders. American Journal of Public Health, 99(3), 493-498.
McEachin, J.J., Smith, T., & Lovaas, I.O. (1993). Long-term outcome for children with autism who received early intensive behavioral treatment. American Journal on Mental Retardation, 97, 359-372.
Ozonoff, S., Iosif, A., Baguio, F., Cook, I.C., Hill, M.M., Hutman, T., Rogers, S.J., Rozga, A., Sangha, S., Sigman, M., Steinfeld, M.B., & Young, G.S. (2010). A prospective study of the emergence of early behavioral signs of autism. Journal of the American Academy of Child and Adolescent Psychiatry, 49, 258-268.
Ozonoff, S., Williams, B.J., & Landa, R. (2005). Parental report of the early development of children with regressive autism: The “delays-plus-regression” phenotype. Autism: The International Journal of Research and Practice, 9, 495-520.
Rice, C. (2009). Prevalence of autism spectrum disorders: Autism and developmental disabilities monitoring network, United States, 2006. Morbidity and Mortality Weekly Report. Surveillance Summaries, 58(SS-10), 1-25.
Robins, D.L., Fein, D., Barton, M. L., & Green, J. A. (2001). The modified checklist for autism in toddlers: An initial study investigating the early detection of autism and pervasive developmental disorders. Journal of Autism and Developmental Disorders, 31, 131-144.
Rogers, S.J. (2009). What are infant siblings teaching us about autism in infancy? Autism Research, 2(3), 125-137.
Rogers, S. J. (1996). Brief Report: Early intervention in autism. Journal of Autism and Developmental Disorders, 26, 243-247.
Rogers, S. J., & Lewis, H. (1989). An effective day treatment model for young children with pervasive developmental disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 28, 207-214.
Rutter, M., Le Couteur, A., & Lord, C. (2003a) Autism Diagnostic Interview-Revised (ADI-R). Los Angeles , CA : Western Psychological Services.
Rutter, M., Bailey, A., Lord, C., & Berument, S.K. (2003b). Social Communication Questionnaire. Los Angeles, CA: Western Psychological Services.
Schopler, E., Reichler, R., & Renner, B. (1988). The Childhood Autism Rating Scale (CARS). Los Angeles: Western Psychological Services.
Shattuck, P., Durkin, M., Maenner, M., Newschaffer, C., Mandell, D., Wiggins, L., Lee, L.C. Rice, C., Giarelli, E., Kirby, R., Biao, J., Pinto-Martin, J., & Cuniff, C., (2009). Timing of identification among children with an Autism Spectrum Disorder: Findings from a population-based surveillance study. Journal of the American Academy of Child & Adolescent Psychiatry, 48(5), 474-483.
Sheinkopf, S.J., & Siegel, B. (1998). Home-based behavioral treatment of young children with autism. Journal of Autism and Developmental Disorders, 28(1), 15-23.
Siegel, B. (2004). Pervasive Developmental Disorders Screening Test II manual. Minneapolis: NCS Pearson, Inc.
Siperstein, R., & Volkmar, F. (2004). Brief report: Parental reporting of regression in children with pervasive developmental disorders. Journal of Autism and Developmental Disorders, 34(6), 731-734.
Smith T., Groen A.D., & Wynn J.W. (2000). Randomized trial of intensive early intervention for children with pervasive developmental disorder. American Journal on Mental Retardation, 105(4), 269–285.
Squires, J., Bricker, D., & Twombly, E. (2002a). Ages & Stages Questionnaires: Social-Emotional: A parent completed, child-monitoring system for social-emotional behaviors. Baltimore, MD: Paul H. Brookes Publishing Co., Inc.
Stone, W.L., Coonrod, E.E., & Ousley, O.Y. (2000). Screening tool for autism in two-year-olds (STAT): Development and preliminary data. Journal of Autism and Developmental Disorders, 30, 607-612.
Stone, W.L., Coonrod, E.E., Pozdol, S.L., & Turner, L.M. (2003). The Parent Interview for Autism – clinical version (PIA-CV): A measure of behavioral change for young children with autism. Autism, 7, 9-30.
Stone, W.L., Lee, E.B., Ashford, L., Brissie, J., Hepburn, S.L., Coonrod, E.E., & Weiss, B.H. (1999). Can autism be diagnosed accurately in children under 3 years? Journal of Child Psychology and Psychiatry, 40(2), 219-226.
Turner, L.M., & Stone, W.L. (2007). Variability in outcome for children with an ASD diagnosis at age 2. Journal of Child Psychology and Psychiatry, 48(8), 793-802.
Werner, E., & Dawson, G. (2005). Validation of the phenomenon of autistic regression using home videotapes. Archives of General Psychiatry, 62-68, 889-895.
Werner, E., Dawson, G., Munson, J., & Osterling, J. (2005). Variation in early developmental course in autism and its relation with behavioral outcome at 3–4 years of age. Journal of Autism and Developmental Disorders, 35(3), 337-350.
Wetherby, A.M., & Prizant, B.M. (2002). Communication and Symbolic Behavior Scales Developmental Profile Manual, first normed edition. Baltimore: Paul H. Brookes.
ZERO TO THREE. (2005). Diagnostic classification of mental health and developmental disorders of infancy and early childhood (Rev. ed.; DC: 0–3R). Washington, DC: ZERO TO THREE Press.